PCL Avulsion Injuries
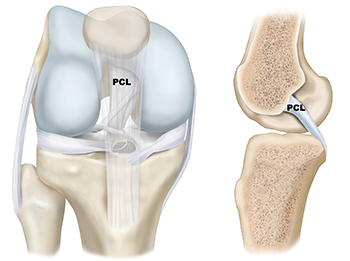
There are three bones that make up the knee joint – the femur (thigh bone), the tibia (shin bone), and the patella (kneecap). There are two cruciate ligaments—Posterior Cruciate Ligament (PCL) and Anterior Cruciate Ligament (ACL)—inside the knee joint that cross to form an X. The PCL sits in the back of the knee joint, while the ACL sits in the front of the knee joint. Together, they help control the front-to-back motion of the knee, as well as rotation.
The PCL is one of two cruciate ligaments in the knee joint that cross to form an X. It is a vital structure that helps stabilize the knee and control its movement. The PCL is the largest and strongest ligament in the knee. It has two very distinct portions: one that goes from the back of the tibia to the roof of the femoral notch (in the thigh bone) called the anterolateral bundle, and a second smaller portion that goes to the side of the notch called the posteromedial bundle. Both bundles work together to prevent the knee from slipping backward, especially when it is bent.
Recall that the PCL has two bundles: the anterolateral bundle and the posteromedial bundle. The anterolateral bundle prevents excessive front-to-back motion of the tibia while the posteromedial bundle prevents excessive rotation of the tibia.
Two important structures associated with the PCL are the meniscofemoral ligaments. These are small ligaments that can sometimes be found in the knee joint. These structures attach to the lateral meniscus and follow a similar course alongside the PCL in order to attach to the femur. One of meniscofemoral ligaments attaches in the front of the posterior cruciate ligament (Ligament of Humphrey’s) and the other attaches in the back (Ligament of Wrisberg). The anterior one is present in 30% of patients and the posterior one is found in 60% of knees. Both ligaments help the PCL and prevent the knee from slipping backwards.
Given the PCL’s size and strength, it takes a significantly traumatic injury to tear it. Consequently, a PCL tear by itself, called an isolated PCL tear, is not that common. Instead, PCL injuries are usually associated with other ligamentous injuries (MCL, LCL or ACL) or meniscal injuries. Most isolated PCL tears occur as a result of an injury to the front of the knee when it is bent. Falling on a bent knee while playing sports, slipping on ice, or hitting a dashboard during a traffic accident are some common ways that the PCL is injured.
While the majority of PCL injuries are intrasubstance tears, a small subset of injuries involves avulsion fractures off the femoral or tibial attachment of the PCL. PCL avulsion fractures at the femoral attachment are much less common than tibial-sided avulsion fractures.
Patients can present with swelling, discomfort, and pain, typically when the knee is bent. When combined injuries are diagnosed, severe instability can be present. In these cases, arteries or nerves can be compromised, and therefore, it is important to rule these injuries out.
The combination of a detailed history, comprehensive physical examination, x-rays, and an MRI (magnetic resonance imaging) is the key to a successful diagnosis of a PCL avulsion injury. Dr. Jorge Chahla and his team use stability tests as part of the physical exam, including the Posterior Drawer test, Supine Internal Rotation (IR) test, quadriceps active tests, and degree of posterior sag to properly diagnose a PCL Injury.
Because isolated PCL avulsion injuries are rare, imaging studies, such as an MRI, are important to evaluate the full extent of your injuries and rule out concomitant ligamentous or meniscal injuries.
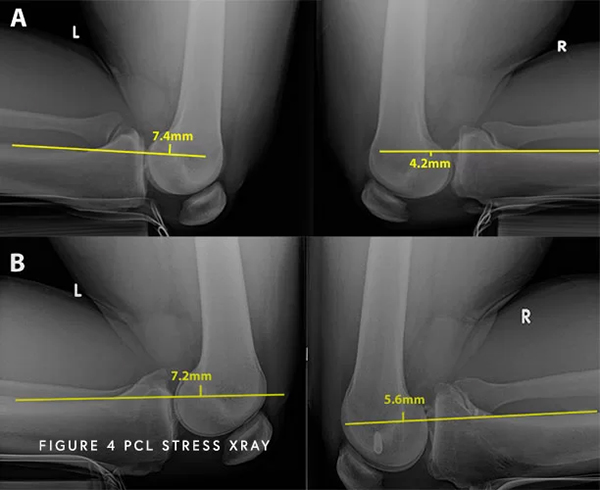
Moreover, to help evaluate the functionality of the injured PCL, a special test called kneeling stress x-rays may be ordered to determine the severity of your PCL injury. These special x-rays allow for objective quantification and diagnose (based on validated systems) of a partial, complete, or combined PCL injury with millimeter accuracy. With this information, Dr. Chahla can provide an accurate diagnosis and treatment plan.
A posterior cruciate ligament (PCL) avulsion injury occurs when the ligament is torn away from the bone, often resulting from high-impact trauma. This injury can cause knee instability, pain, and difficulty with movement. Dr. Jorge Chahla, a specialist in knee ligament injuries, offers expert evaluation and treatment for PCL avulsion injuries. If you suspect a PCL injury, schedule an appointment with Dr. Chahla in Chicago, Naperville, or Oak Brook to determine the best course of treatment.
At a Glance
Dr. Jorge Chahla
- Triple fellowship-trained sports medicine surgeon
- Performs over 700 surgeries per year
- Associate professor of orthopedic surgery at Rush University
- Learn more