Rotator Cuff Tears
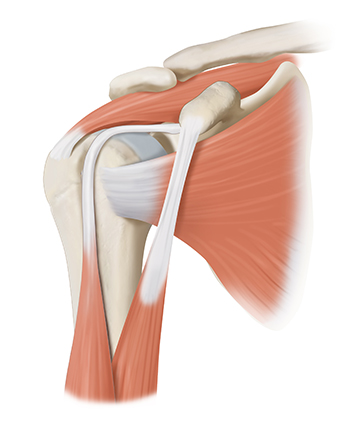
The shoulder is made up of two joints, the acromioclavicular joint and the glenohumeral joint. The glenohumeral joint is a ball and socket joint. The socket is the flat, shallow surface called the glenoid, and the head of the humerus is the ball. The joint capsule is a fluid-filled sac that surrounds the shoulder joint and provides lubrication for shoulder joint movement. The rotator cuff connects the humerus to the scapula and is made up of the tendons of four muscles, the supraspinatus, infraspinatus, teres minor and the subscapularis. These muscles and tendons provide strength and stability to the shoulder joint, supporting overhead and other arm motions necessary to perform daily tasks and activities.
A rotator cuff tear can cause shoulder pain, weakness, and difficulty lifting the arm, making everyday activities challenging. These tears often result from injury, overuse, or age-related degeneration. Dr. Jorge Chahla, a highly experienced orthopedic shoulder surgeon, provides comprehensive diagnosis and treatment for rotator cuff injuries, helping patients restore shoulder strength and function. If you have persistent shoulder pain, schedule an appointment with Dr. Chahla in Chicago, Naperville, or Oak Brook for expert evaluation.
- Triple fellowship-trained sports medicine surgeon
- Performs over 800 surgeries per year
- Associate professor of orthopedic surgery at Rush University
- Learn more