Two-Stage Revision Anterior Cruciate Ligament Reconstruction with Cannulated Allograft Bone Dowels Soaked in Bone Marrow Aspirate Concentrate
Anterior cruciate ligament reconstruction (ACLR) is one of the most common orthopedic procedures performed each year. The majority of patients undergoing these reconstructions will experience long-term stability and symptomatic relief, however, some will require a revision ACLR procedure. In general, revision ACLRs are more challenging than primary ACLRs due to several diagnostic and technical considerations. A revision ACLR can be performed with either a one-stage or two-stage procedure, which is based on the presence or absence of malpositioned tunnels, bone loss, and tunnel expansion. Recently, the introduction of pre-shaped allograft bone dowels as a bone grafting option has gained popularity. They provide immediate structural stability and avoid donor site morbidity associated with autografts. The purpose of this paper is to outline a bone grafting tunnel technique with cannulated allograft bone dowels soaked in bone marrow aspirate concentrate (BMAC) used in the first stage of a staged revision ACLR procedure.
Authored
- Luc M. Fortier, BA
- Safa Gursoy, MD, PhD
- Harsh Singh, BA
- Jorge Chahla, MD, PhD
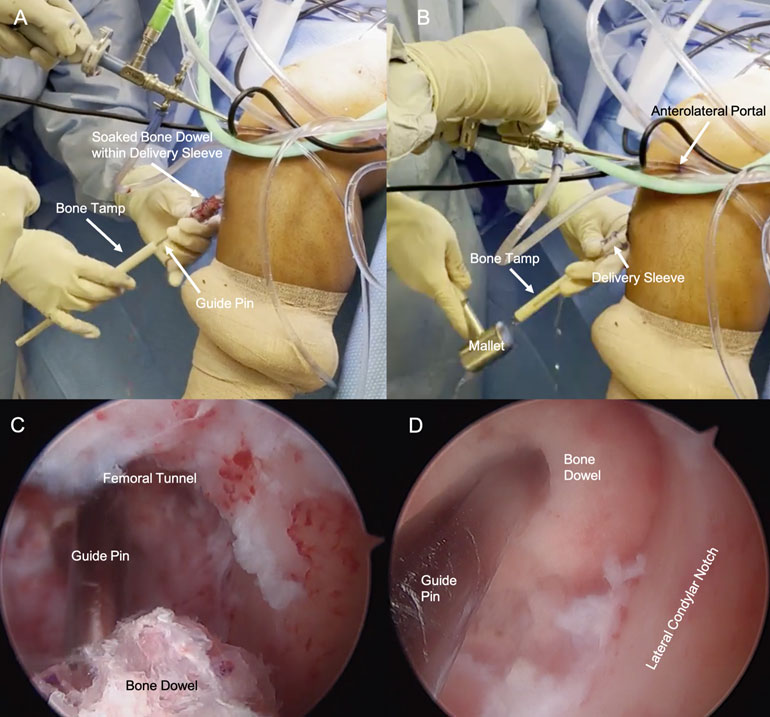
Placing the bone dowel into the femoral tunnel in a left sided patient. While maintaining 90 degrees of left knee flexion, the cannulated bone dowel soaked in bone marrow aspirate concentrate (BMAC) is inserted over the guide pin and into the delivery sleeve. The bone tamp is then inserted through the delivery sleeve behind the bone dowel (A). The bone tamp is used to advance the bone dowel into the joint space. A mallet is used to gently impact the tamp (B). Arthroscopic visualization through the anteromedial portal confirms advancement of the 10 mm bone dowel (C). Arthroscopic visualization through the anteromedial portal confirming the 10 mm cannulated bone dowel soaked in BMAC sits slightly proud within the femoral tunnel (D).
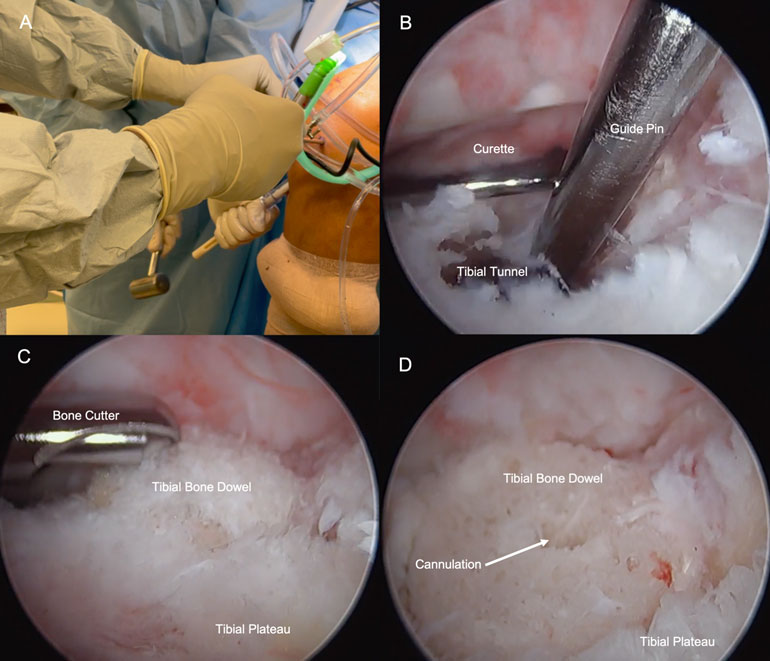
Placing the bone dowels into the tibial tunnel in a left sided patient. Mallet is used to gently impact the bone tamp as it advances the 12 mm bone dowel into the tibial tunnel of the left knee (A). While the bone dowel is advanced into the defect, a large curette is inserted through the anteromedial portal and placed above the proximal tibial tunnel opening to provide a roof and avoid advancing the bone dowel too far into the joint space (B). Arthroscopic visualization through the anterolateral portal of the bone cutter utilized to contour the proud edges of the bone dowel to sit flush against the surface of the tibial plateau (C). Arthroscopic view through the anterolateral portal of the bone dowel sitting within the tibial tunnel after bone cutter was used to contour the proud edges (D).
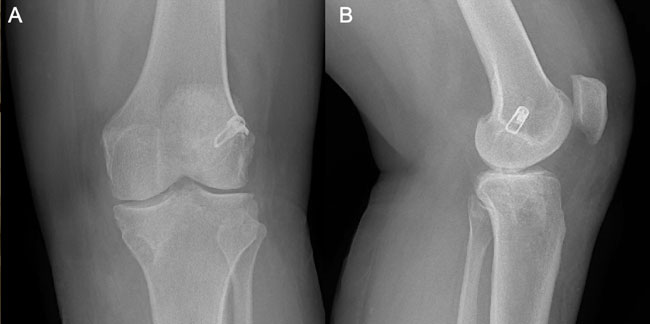
Postoperative anteroposterior (AP) radiograph of the left knee (A). Postoperative lateral radiograph of the left knee (B).
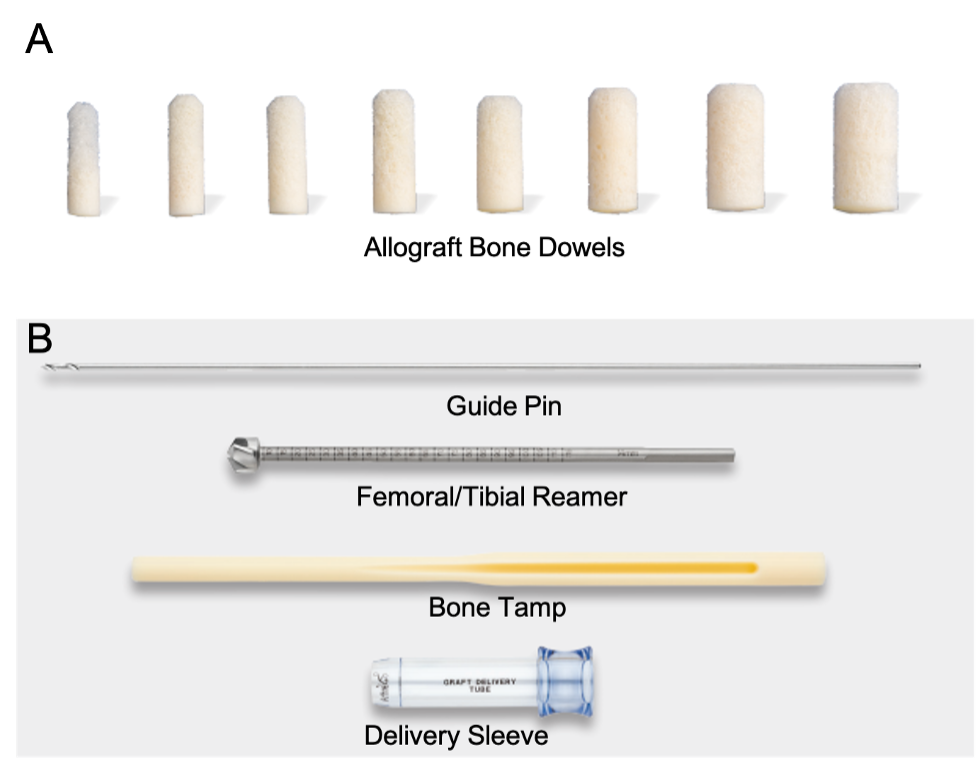
Arthrex cannulated allograft bone dowels with tapered end; readily-available in different sizes to correspond with size of defect (A). Corresponding instrumentation used to insert the bone dowel, including 2.4 mm guide pin, femoral/tibial reamer, bone tamp, and delivery sleeve (B).